
August 18, 2023
4 min read
Clinical pearls for frontline PCPs
An 83-year-old woman presents to the office for evaluation of dizziness.
She has noted dizziness off and on for the past 2 to 3 years. Although she has difficulty describing the dizziness, she calls it a “faint feeling” and notes it primarily when she gets up too fast. It usually is noted in the morning.
Two days ago, she began noting a much different type of dizziness. It began when she rolled over in bed and described it as severe room spinning. She has been miserable for the past 2 days with the dizziness and the nausea and vomiting that has accompanied it. She has not been able to do any of her activities of daily living and has not ventured outside of her apartment since the spinning sensation began. She is brought to the office by a friend.
The patient’s past medical history includes hypertension, chronic neck pain and mild depression. Her medications include lisinopril, amlodipine and acetaminophen.

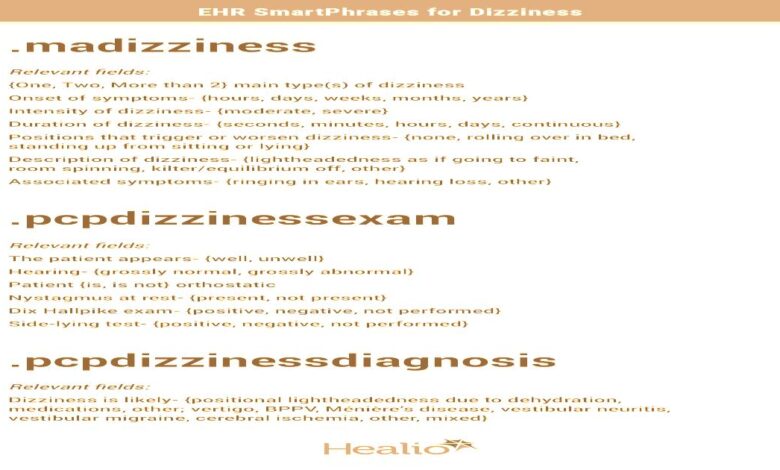
The medical assistant (MA) checks the patient in, offers her an emesis basin and performs orthostatic BP and heart rate measurements in the lying and standing position. Her hearing is good. She looks slightly pale. He asks her numerous pertinent questions and records the answers using the SmartPhrase “.madizziness.”
He reviews the case with the primary care physician:
“Doc, this 83-year-old female patient feels miserable. She has a 2- to 3-year history of chronic dizziness or lightheadedness as if she were going to faint when she gets up too fast. About 2 days ago, she developed another very different type of dizziness — severe room spinning that she first noted after she rolled over in bed. This has been associated with nausea and vomiting. She has felt so lousy that she has not been able to go out of her apartment. She just looks miserable. I did orthostatics, and her BP lying down was 110 mm Hg/70 mm Hg with a heart rate of 80. When I stood her up for 2 minutes, her BP dropped to 85 systolic and her heart rate went to 100. She got very dizzy when she stood up. She is worried that something is very wrong.”

The PCP reviews the MA’s documentation and enters the room. The patient looked pale and miserable. Her skin turgor was decreased, and her mucous membranes were very dry. Her physical exam showed a normal cardiac exam except for mild tachycardia. No nystagmus was noted. The PCP was considering a Dix Hallpike test but decided against doing it because of her history of chronic neck pain and her diminished cervical spine range of motion. He performed the side-lying test, which was strongly positive on the right and negative on the left.
He suspected a peripheral cause of her vertigo. He gave her 8 mg of sublingual ondansetron for the nausea. He performed the Epley canalith repositioning maneuver, and her symptoms improved by about 75%. He then referred her to vestibular rehabilitation in physical therapy. He ordered a CBC and BMP, which both came back normal. He recommended that she increase her fluid intake and asked her to stop her amlodipine and to switch her lisinopril to bedtime.
The PCP saw her back in 1 month for an annual wellness visit. Her BP was 140 mm Hg/80 mm Hg. She did not have any further room spinning and her chronic positional lightheadedness had improved significantly.
Lessons Learned:
- Major causes of chronic dizziness include positional lightheadedness, vertigo, disequilibrium, other (eg, anxiety, panic disorder) and mixed.
- The most common cause in older patients is mixed-multiple etiologies.
- The Dizziness Handicap Inventory can be a helpful tool for patients to fill out prior to having the PCP evaluate the patient.
- Look for medications that could contribute to positional lightheadedness, and either reduce the dose, stop it altogether or switch to having the patient take it at bedtime.
- Diagnose benign paroxysmal positional vertigo (BPPV) by doing the Dix Hallpike maneuver. If the patient has chronic neck pain and/or diminished cervical spine range of motion, you could do a side-lying test. Another helpful bedside test is the HINTS test, a useful method to differentiate benign peripheral conditions from central nervous system lesions like strokes.
- Become familiar with and treat BPPV with the Epley canalith repositioning maneuver. It is remarkably effective.
- Vestibular rehabilitation (usually performed in physical therapy) can be useful for all types of dizziness.
- Ask the patient open-ended questions to allow the patient to better describe what they mean by dizziness. Inquire about timing, intensity and duration of symptoms. Ask if symptoms occur in different positions.
- Avoid long-term use of vestibular suppressing agents and antinauseants — ie, limit their use to no more than 3 consecutive days as long-term use can cause the brain to habituate. Recent studies suggest that vitamin D3 can be helpful in reducing recurrence of BPPV, so that could be considered as a supplement.
- SmartPhrases are time-saving tools in the electronic health record that can pull together long phrases or paragraphs into a note. They can standardize the approach and help users to recall key concepts of evaluation, history and physical as well as patient information. The phrases can be built by your informatics specialist. Relevant smartphrases for chronic dizziness include .madizziness, .pcpdizzinessexam, .pcpdizzinessdiagnosis and .avsdizziness.



